
Watch an exclusive video of Dr. Bruce E. Johnson delivering his Presidential Address at the 2018 ASCO Annual Meeting. Read the transcript of his address below the video.
As I present on the theme of my presidential year—"Delivering Discoveries: Expanding the Reach of Precision Medicine”—I do it from the perspectives of a clinician, an academic physician, and perhaps with a perspective that gives me insight into our profession, as a cancer survivor.
There is no question that we are witnessing a transformation of cancer care brought about by precision medicine. All of us in this room are fortunate to be in this field—and be part of this time of dramatic innovation in cancer research and treatment. But if we are going to expand the reach of precision medicine, there is still a lot for us to do. Today, I’ll talk about insights from the past, how these insights inform the opportunities before us, and how all of us can continue to advance this field.
First, it’s important to note that precision medicine is about improving our patients’ lives, so that they can not only live longer, but can live much better. My own experience working in lung cancer for 35 years has allowed me to both participate in the research and personally apply the principles of precision medicine for my patients. You will hear from two of them later in my talk.
Today, I’d like to talk about how this revolution in precision medicine has occurred and lessons learned from the past. While the success of precision medicine may seem like an overnight success, it has actually been a thoughtful, strategic approach based on decades of hard, disciplined work by dedicated scientists around the world. The success in lung cancer has resulted in:
- Identifying lung cancer’s first oncogene that can be effectively treated with targeted agents
- Identifying more oncogenes leading to even more treatment options with effective targeted therapies
- Immunotherapy coming of age, which is playing a pivotal role in the treatment of many patients with lung cancer
The cumulative effect of these efforts has been transformative, and the effect has been observed clinically in less than a decade and a half.
Today, nearly half of all patients presenting with lung cancer can now be initially treated with targeted agents or immunotherapy rather than chemotherapy—half of all patient with advanced lung cancer, about 70,000 a year. And there’s more to come. Precision medicine is impacting the lives of people living with cancer, including myself, not only in terms of survival, but also in terms of us being able to experience important and memorable events in our lives.
This revolution in cancer therapy is especially impressive when one considers the state of thoracic oncology a short 16 to 18 years ago. At that time, investigators from a cooperative group here in the United States carried out a study for patients with advanced non-small cell lung cancer (NSCLC). They compared four different chemotherapy regimens considered at that time to be promising. The study was considered so important at that time, it was presented at the Plenary Session at the ASCO Annual Meeting in 2000 and published 2 years later in the New England Journal of Medicine.
I share this example for several reasons. First, because it shows that the patient characteristics that are now considered critical to managing patients were not even reported in the publication. For example, the manuscript didn’t list the histology: adenocarcinoma, squamous cell, or large cell carcinoma! Everything was lumped into a single category of non-small cell lung cancer. Also, there was no information on cigarette smoking in the table of patient characteristics. Why? Because in 2002 that wasn’t considered important in assessing patients and formulating their treatment plans.
Contrast it to today: whether a patient smokes is now one of the most important pieces of information in their patient history. This is because patients who don’t smoke are more likely to have genomic changes that can be targeted by existing treatments and patients who do smoke are more likely to respond to immunotherapy.
Just to show you how far we’ve come, a study showing no difference in outcomes with median survivals of just 8 months was considered important enough to be presented at our Plenary Session at ASCO in 2000 and to be published in the New England Journal of Medicine in 2002!
Thankfully, things have changed. Today I’m going to briefly touch upon how we got here, and where we still need to go.
In my area of research, lung cancer, precision medicine is indeed transforming the treatment of this disease—and has important implications for other cancers and for the future of our patients with cancer. Today’s achievement of being able to systematically identify genomic changes that can be successfully targeted goes back nearly 15 years. And it underscores the importance of well-annotated preclinical models that have played a part in this exciting journey. It’s also one of the early examples of team science that began to transform the treatment of lung cancer a decade and a half ago.
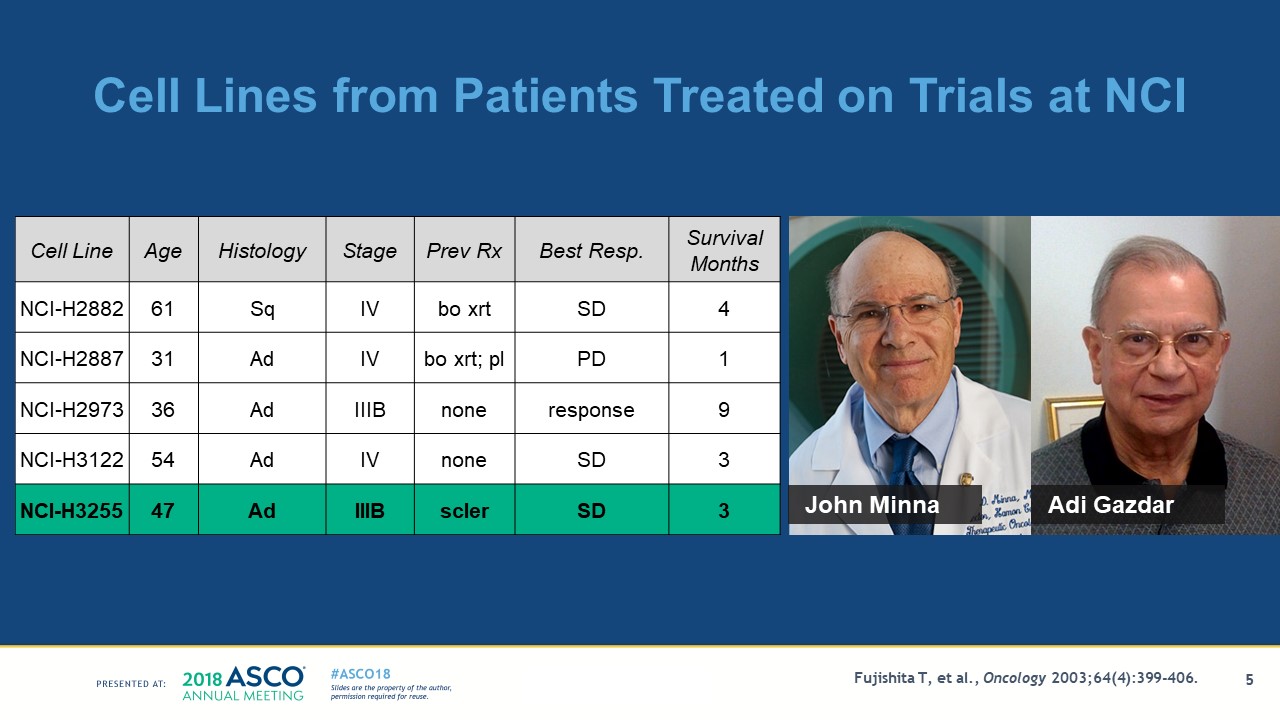
Two of the leaders in this area, Drs. John Minna and Adi Gazdar, were colleagues and mentors at the National Cancer Institute. They led the effort to generate the tumor cell lines from patients with lung cancer treated on our clinical trials. My own contribution was to help annotate the clinical histories of these patients who participated in the trials whose tumors gave rise to permanent cell lines. Generation of these annotated cell lines allowed us to hone in on those tumor cell lines likely to be sensitive to the targeted agents.
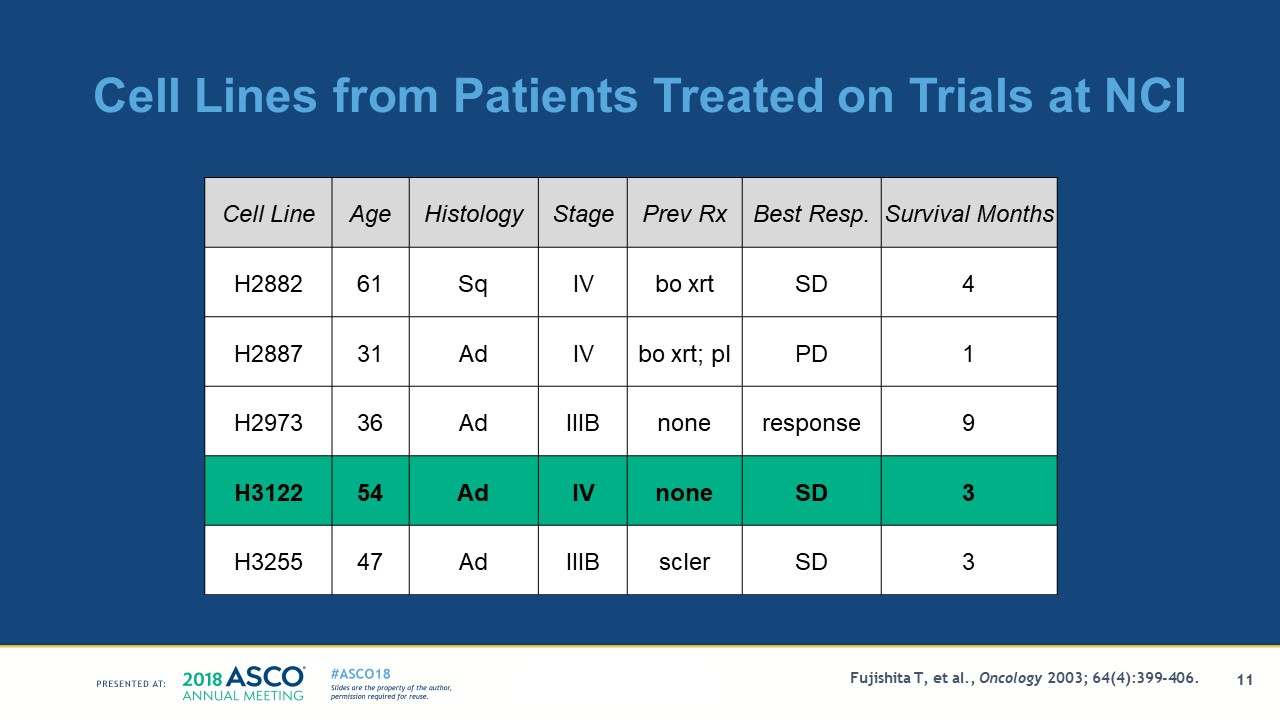
The critical clinical observations made by 2004 were that never-smoking women with adenocarcinoma and patients with lung cancer from East Asia were more likely to respond to the targeted agents against the epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) gefitinib and erlotinib. The table below, taken from one of our publications, depicts the patients’ age, histology, stage, treatment status, and their survival from the start of protocol therapy. Although not shown in this table, their smoking status and gender were collected as well. I have highlighted NCI-H3255 in teal, a cell line from a woman with adenocarcinoma who didn’t smoke—and I’ll talk about the properties of the cell line later.
By linking the clinical characteristics with the people who respond to gefitinib and erlotinib and the characteristics of the cell line model, we were able to observe similar biological behavior both in patients and in the preclinical model. By studying these annotated tumor cell lines, we were able to show the preclinical models were more sensitive to this class of drugs, gefitinib in this case.
The clinical observations prompted me to retrieve the preclinical model H3255. It was established from a woman with adenocarcinoma who had never smoked, information known from the annotation, so we believed the cell line was more likely to be sensitive to the EGFR-TKI gefitinib.
The growth of the cell line highlighted, H3255, is shifted to your left, meaning the cell line is 100-fold more sensitive to gefitinib than the other cell lines. My colleague, Dr. Pasi Janne, discovered a DNA mutation in EGFR, now referred to as L858R. Other colleagues, Drs. Matthew Meyerson and William Sellers, sequenced the same domains in EGFR as studied in the cell line in more than 100 lung cancers.
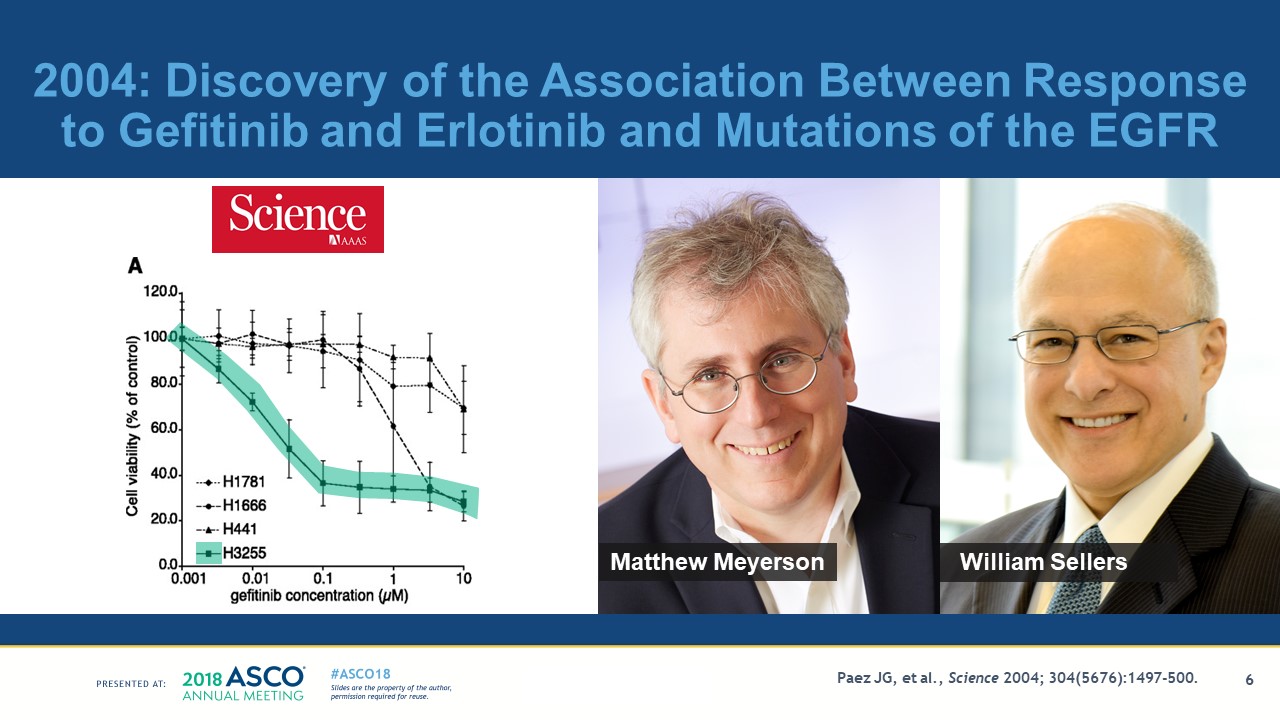
They discovered the same EGFR mutation detected in H3255 in three different adenocarcinomas of the lung in patients from Japan, a country where clinical observations showed patients were three times more likely to respond to gefitinib or erlotinb than patients from the United States.
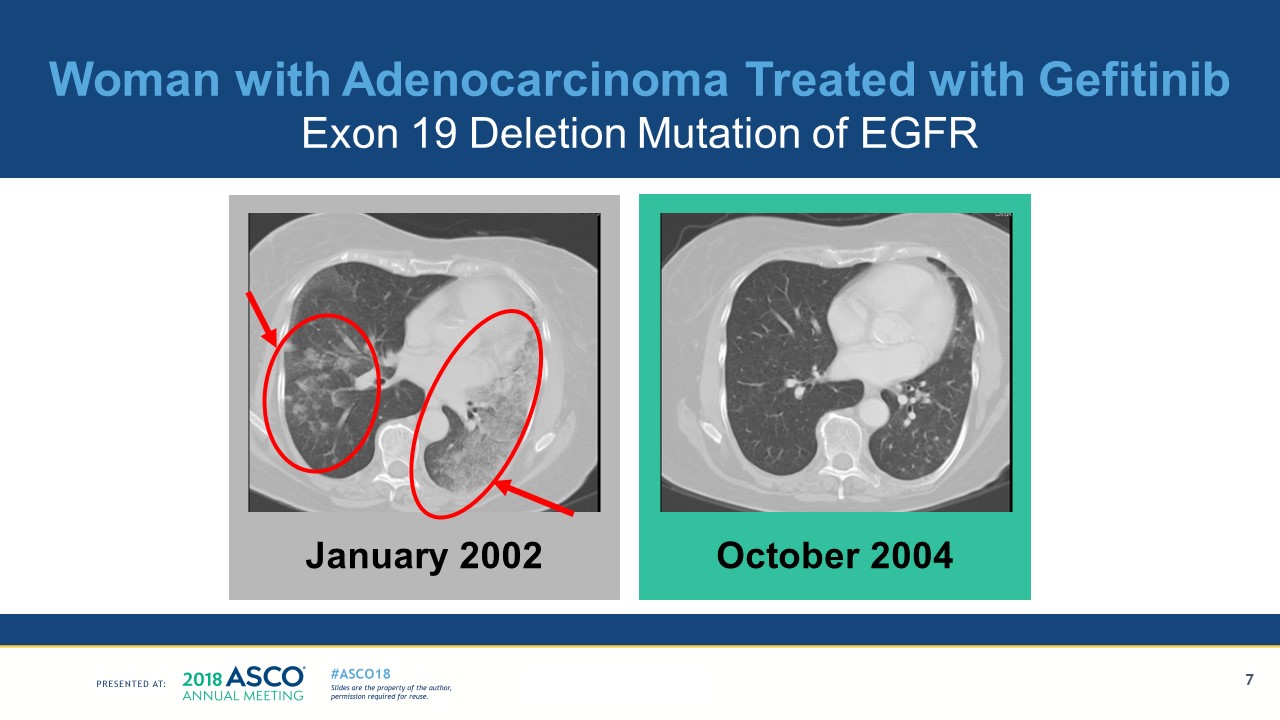
The findings from studying the preclinical models prompted us to study the patients with exceptional responses to gefitinib. Lung cancers were identified from five patients treated at the Dana-Farber Cancer Institute who had dramatic responses to treatment with either gefitinib or erlotinib. One of our first exceptional responders was a patient whose tumor responded for more than 2 years while being treated with gefitinib. The CT scans of the patient are shown below, with bilateral tumor infiltrates that resolved on gefitinib shown in the right panel.
All five of the tumors studied from the patients whose tumors responded to gefitinib had mutations in the tyrosine kinase domain of EGFR, while the four patients who did not respond to the EGFR-TKI had a wild-type receptor. These observations ultimately contributed to a dramatic shift in the treatment of some patients with lung cancer.
Two other laboratory groups, led by Drs. Thomas Lynch and Daniel Haber at Massachusetts General Hospital and Drs. William Pao and Harold Varmus at Memorial Sloan Kettering, made observations in 2004 showing that a total of 25 of 31 patients who responded to gefitinib or erlotinib had sensitizing mutations of EGFR while those without mutations did not respond. These findings have transformed lung cancer care and these three manuscripts have now been referenced more than 24,000 times.
Fourteen years later, there are now four different EGFR-TKIs approved in the United States and around the world for patients with lung cancer with mutations of EGFR. Importantly, it is part of the initial treatment for approximately 15% of patients with non-small cell lung cancer here in the United States—and their outcomes are much better than those treated with chemotherapy. Patients with these EGFR mutations are likely to live for 2.5 years from their diagnosis of metastatic lung cancer while those without the mutation treated with chemotherapy survive for less than half the time, about a year. The testing for mutations in the EGFR receptor in patients with advanced nonsquamous non-small cell lung cancer now takes place around the world and is a part of routine care for more than 85,000 patients in the United States.
The first genomic change that could be effectively targeted was the EFGR mutation, which was discovered because:
- The L858R mutation is present in preclinical cell line models that are sensitive to gefitinib.
- Patients who responded to gefitinib had the same L858R mutation as the sensitive cell line.
- Those who did not respond did not have the mutation.
- In Asian patients with adenocarcinoma of the lung where the clinical responses are more frequent, the L858R mutation was more frequent as well.
The successful targeting of the first oncogenic driver in lung cancer prompted further studies around the world to find additional genomic changes that can be effectively targeted.
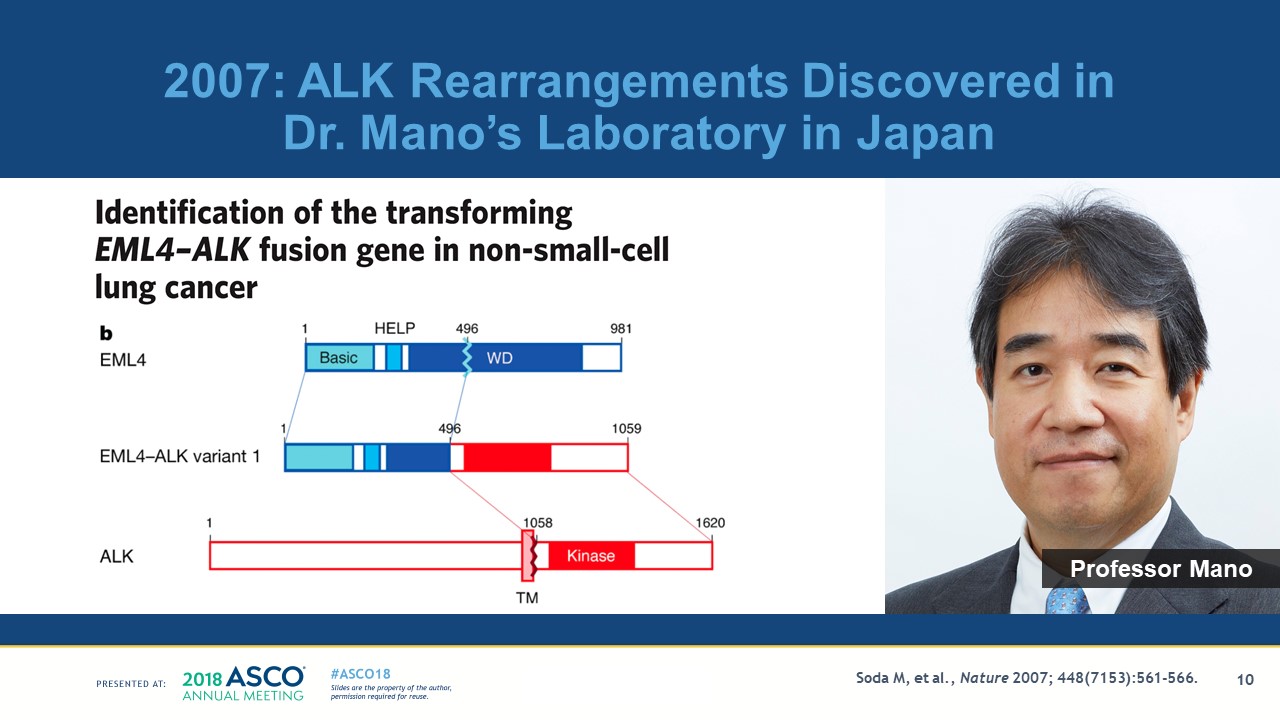
Professor Hiroyuki Mano led the studies that identified the next oncogenic driver in lung cancer to be successfully targeted. Investigators in his laboratory discovered the transforming EML4-ALK fusion gene in five patients with non-small cell lung cancer in 2007; the rearrangement is depicted below. ALK stands for anaplastic lymphoma kinase, because it was initially discovered more than 20 year ago to be translocated in anaplastic lymphomas of childhood. The presence of the translocation in both the anaplastic lymphomas and lung cancers provided compelling evidence that ALK likely played a critical role in the malignant transformation to lung cancer and lymphoma and also identified a potential target for therapy.
The preclinical models were once again central for characterizing the potential therapeutic target and the clinical characteristics of the patients from whom these cell lines were critical for identifying the appropriate models to study. NCI-H3122 is depicted in teal below and was established from a woman non-smoker with adenocarcinoma similar to the patient population in which ALK rearrangements are found. The cell line tested positive for an ALK rearrangement which facilitated additional preclinical studies.
Dr. Janne studied more than 300 tumors and tumor cell lines. 3122 was identified as being sensitive to a drug directed against ALK that eventually became the FDA-approved drug ceritinib. The preclinical xenograft model 3122 shows tumor regressions with increasing doses of the agent directed against the rearranged ALK. Dr. Ultan McDermott in Dr. Jeffrey Settleman’s laboratory led similar studies with the same drug as well as crizotinib in lung cancer cell lines with ALK rearrangements. The preclinical studies showing dramatic antitumor activity against appropriate cell lines and xenograft models prompted the development of a crizotinib as an agent that has been shown to effective for ALK-positive NSCLC and its eventual FDA approval for use in ALK-positive NSCLC in 2011.
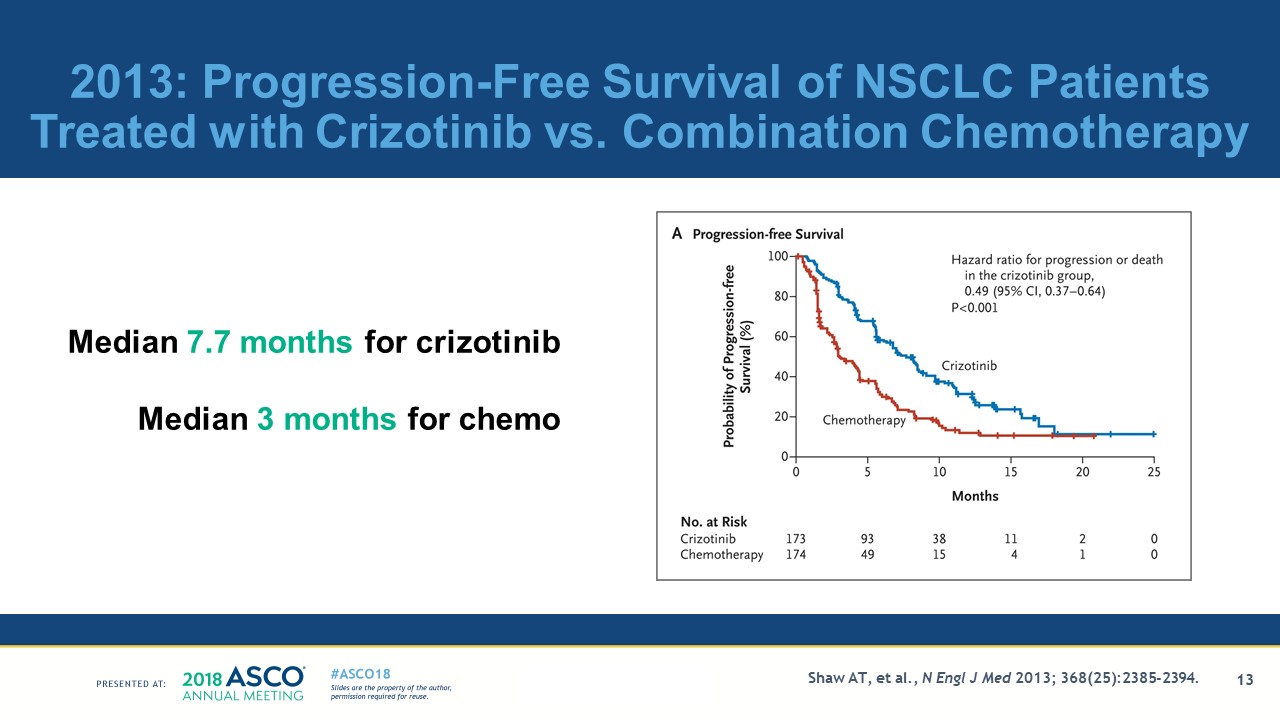
A trial comparing the outcomes of ALK-positive treated NSCLC patients who were given either crizotinib versus single-agent chemotherapy was reported in 2013. The slide below depicts the 2-fold prolonged progression-free survival of the patients treated with crizotinib, median 7.7 months, versus those treated with chemotherapy, median 3 months.
We as oncologists are continually exposed to response rates, and progression-free and survival curves. However, the ultimate test should be whether the targeted agents make our patients feel better while living longer.
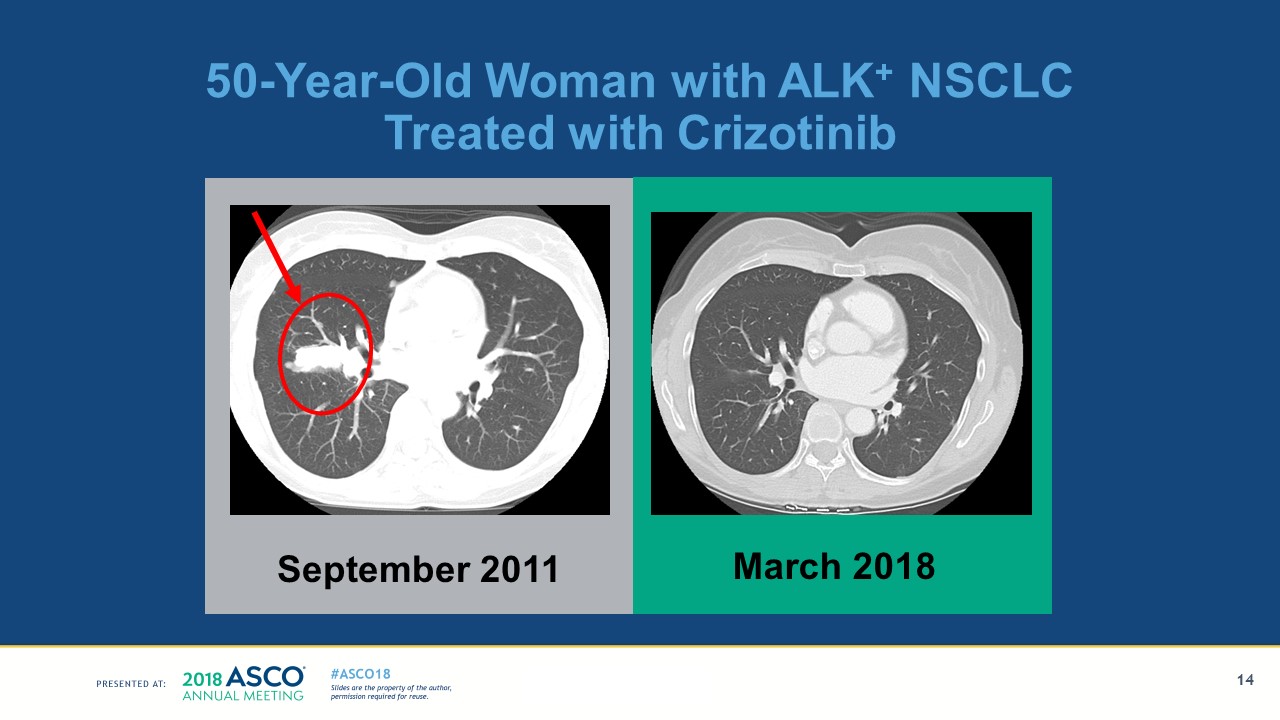
Among those patients with ALK-positive NSCLC who respond to the targeted agent crizotinib, and now other ALK-directed agents, there are patients whose responses now go on for years and have a dramatic impact on their lives. Below are the images of one of my patients who participated in the clinical trial just mentioned. You can see her right-sided lesion on the left panel has resolved and she has been in remission for longer than 6 years.
We commonly think of our interventions in terms of responses, progression-free survival, or overall survival, but one must keep in mind that we are actually trying to make our patients live longer and better lives, one of the principles of precision medicine. Loretta Benkert embodies this principle and she is willing to share her experience and the milestones she has been able to share with her family as she survives her lung cancer and is a beneficiary of precision medicine.
Now, instead of lumping all patients into one group of “non-small cell lung cancer” as we did as late as 2002, we need to apply our principles of precision medicine and identify different genomic changes that prompt different therapies. I am pleased to say today there are now four different oncogenic drivers for which there are FDA- and EMA-approved targeted therapies. These include EGFR, which makes up 15% of patients, and ALK, which makes up another 5% of patients. Crizotinib for ROS1 was added in 2016, and dabrafenib plus trametinib for V600E BRAF mutations were approved in 2017, each making up another 1%.
The result of this is that today about 22% of patients with lung cancer can now be treated with oral targeted agents as their initial therapy rather than combination chemotherapy. This is a dramatic transformation in the past 14 years when everyone used to be treated with chemotherapy.
However, there remain another 78% of patients who still need effective agents directed against their cancer. NTRK and RET rearrangements are among the newest genomic changes in lung cancer and other malignancies that will likely have effective agents. Trials presented at the ASCO Annual Meeting in 2017 and 2018 will hopefully bring that total to 25% of patients with lung cancer. A robust infrastructure in academia, other settings involved in clinical trials, and ongoing pharmaceutical research will continue to be needed to expand the proportion of patients treated with precision medicine.
But it’s not just precision medicine that is revolutionizing cancer treatment. Immunotherapy has now come of age. While the clinical success of immuno-oncology has been realized in the last 5 to 10 years, it was the result of a determined effort to bring immunotherapeutic discoveries into meaningful treatments for patients with cancer for more than three decades. The basic science discoveries two and three decades ago are now having a dramatic impact on the lives of many of our patients with lung cancer. It is basic science discoveries in immunology that have transformed our field performed by key investigators from around the world.
Professor Tasuku Honjo from Japan identified a surface protein, the programmed cell death receptor now known as PD-1. PD-1 is a negative regulator of immune responses and now a target for the class of agents we call checkpoint inhibitors. Other work done in the early 2000s by Drs. Gordon Freeman and Arlene Sharpe, both from my institutions, and Dr. Lieping Chen identified programmed cell death ligand 1 and 2 (PD-L1 and PD-L2), which also caused negative regulation of the immune responses mediated through PD-1. Their pioneering work led to the generation of the class of therapeutic agents directed against PD-1 and PD-L1 called the checkpoint inhibitors and are now being used throughout the world as anticancer agents. Much of the pioneering work with checkpoint inhibitors took place in patients with melanoma, and those of us working in lung cancer have been informed by their ongoing discoveries and their clinical application.
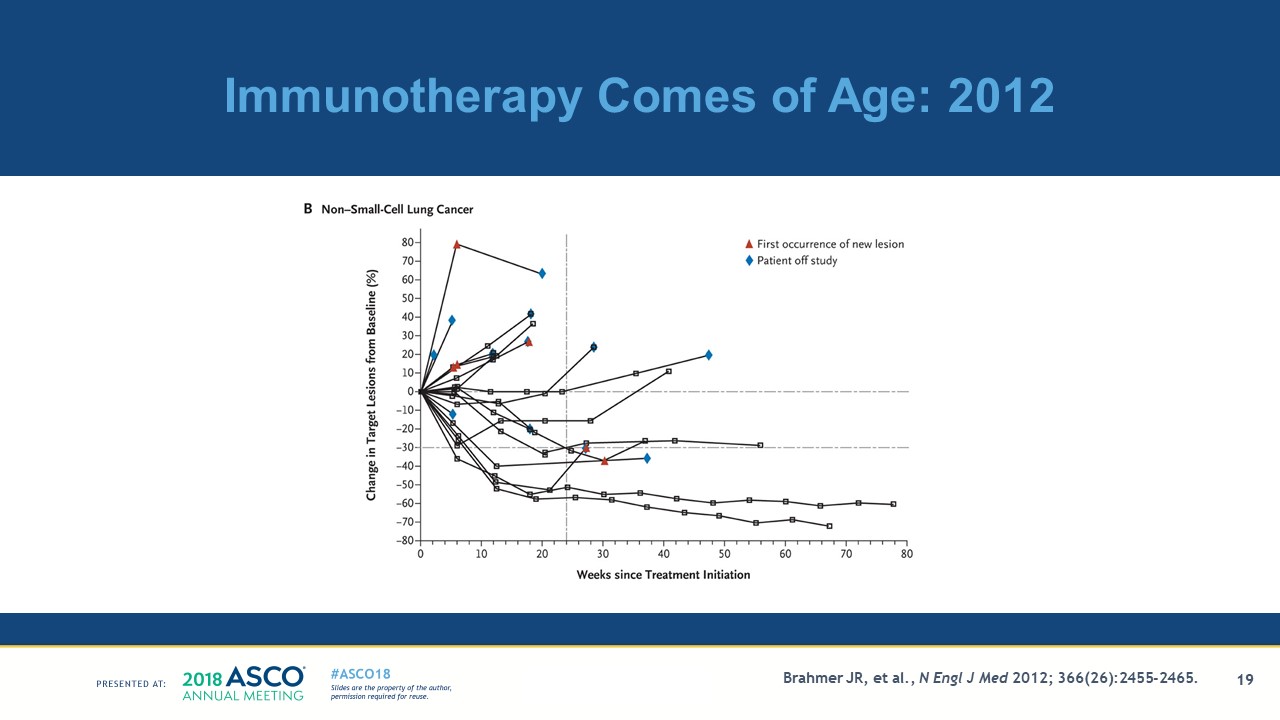
I am happy to say this class of agents, checkpoint inhibitors, are also active in patients with lung cancer. Below I show a spider plot of NSCLC patients’ responses to the checkpoint inhibitor nivolumab, published 6 years ago in 2012. The tumor burden is depicted over time in patients treated with the checkpoint inhibitor nivolumab. There were four of 25 patients with an objective response; these responses were durable for more than 6 months. Importantly, this initial report showed some of these responses appear to go beyond a year.
The 3-year follow-up of studies comparing previously treated patients with NSCLC given the checkpoint inhibitor nivolumab versus docetaxel chemotherapy have now been reported. Their long-term follow-up is encouraging. Patients with previously treated NSCLC are surviving beyond 3 years when treated with the checkpoint inhibitor nivolumab. As shown below, the estimated 3-year survival rates are 17% in the patients with NSCLC and the curve remains relatively flat out toward 5 years. One is gratified that one can speak of 3-year survivals in advanced lung cancer and we await further follow-up.
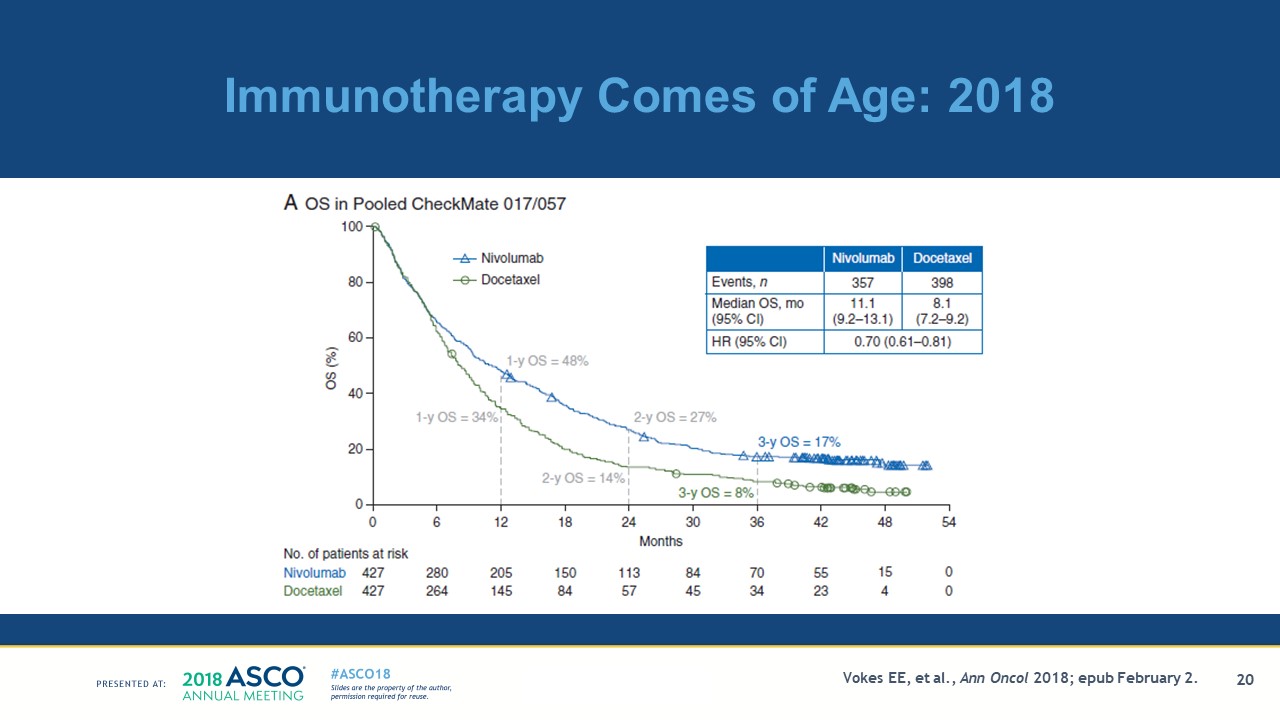
I for one am becoming optimistic that a subset of our patients with lung cancer may actually be cured with checkpoint inhibitor therapy, a finding that is now transforming the treatment of lung cancers. It has been the holy grail of oncology to develop potentially curative treatments for advanced common solid tumors and it may now be on our doorstep for at least some patients.
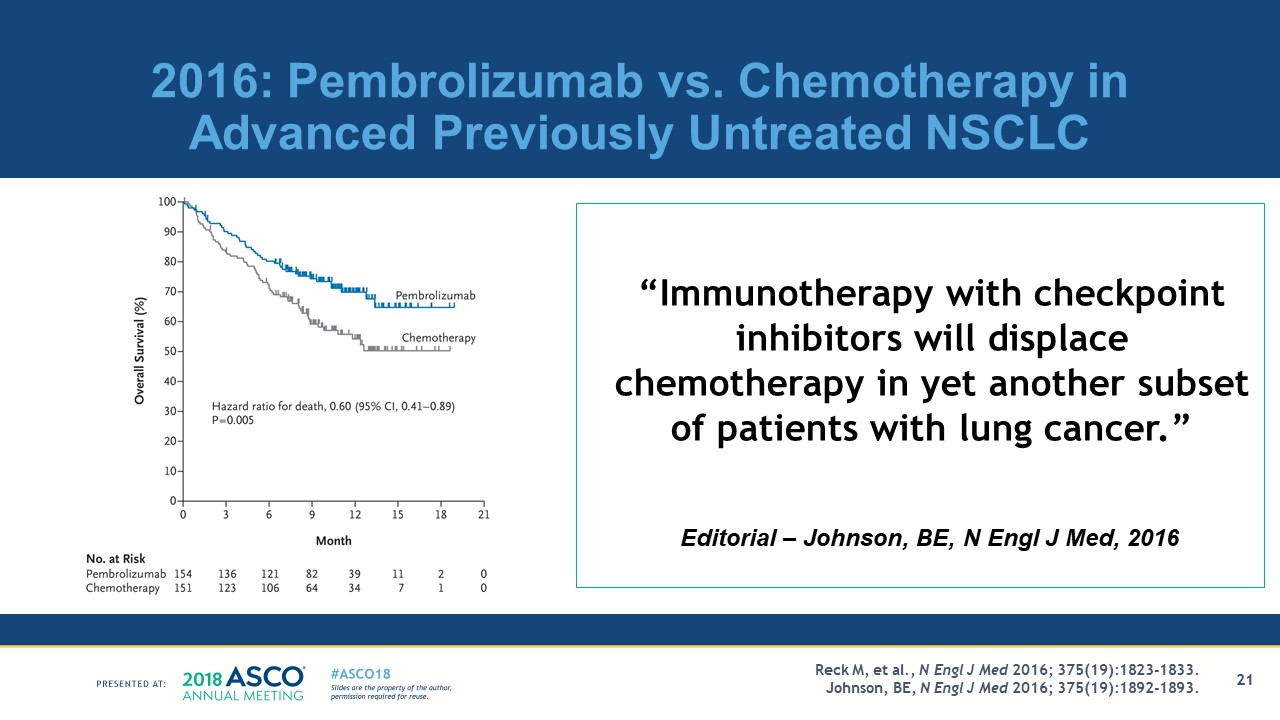
The results of the trial depicted below have also had a dramatic influence on the initial treatment our patients with advanced non-small cell lung cancer. The findings have changed the initial therapy for yet another subset of patients with lung cancer by deploying a predictive marker for the efficacy of a checkpoint inhibitor—patients with untreated advanced NSCLC and PD-L1 expression on at least 50% of tumor cells, which makes up about 25% of the screened patients. The patients were treated with either the checkpoint inhibitor pembrolizumab or platinum-based chemotherapy. The estimated rate of survival at 6 months showed a 40% improvement in survival favoring pembrolizumab. This led to early closure of the trial and the quote in the accompanying editorial: “Immunotherapy with checkpoint inhibitors will replace chemotherapy in yet another subset of patients with lung cancer.”
The results of the trial led to the FDA approval of pembrolizumab for first-line therapy of patients with PD-L1 expression of greater than 50%, about another 25% of the patients with NSCLC. In addition to the 22% of our patients who can be treated with targeted therapies for four different oncogenic drivers, about another 25% of patients can now be initially be treated with a checkpoint inhibitor.
The result is that now in 2018 we are close to being able to treat half of our patients with NSCLC with targeted therapy or immunotherapy as their initial treatment. This is dramatic progress in just a decade and a half. As we enter the era of combination immunotherapy trials, the future becomes even more hopeful.
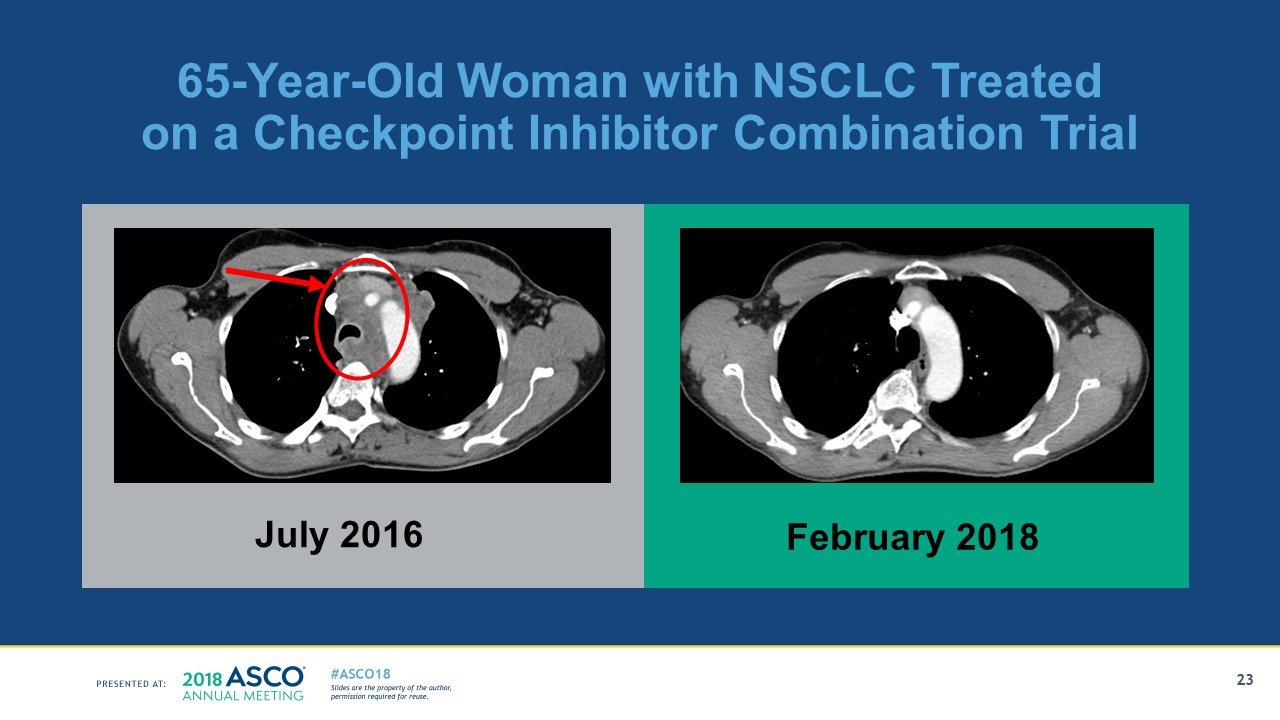
Below are the radiographic images of one of my patients placed on one of the checkpoint inhibitor combination trials. The chest CT scan in 2016 shows the extensive involvement of her mediastinal lymph nodes and tracheal compression and the left-sided chest mass. She started treatment in July 2016 and has a near-complete remission, shown in the right panel. We commonly think of our interventions in terms of responses, as shown in this slide, but as I said before, we must keep in mind that we are actually trying to make our patients live better as well as longer lives.
But instead of me talking about how Elaine is doing that, I’d like Elaine to tell you in her words.
As Elaine has put it much better than me, the delivery of immunotherapy to our patients with advanced cancer can transform their lives, not only in terms of living longer, but also living better.
As I said at the beginning of my presentation, I come to you today not only as an oncologist and cancer researcher but as a person experiencing cancer. My own encounter with prostate cancer has allowed me to see cancer in a very different way than we commonly see it professionally. Knowing how to decide about screening as the son of a patient with prostate cancer and then going through the long wait of evaluation and treatment as a patient myself has been an eye-opening experience. I now share some of the experiences that my patients routinely experience.
My personal exposure to dealing with prostate cancer came when my dad was diagnosed in 2006, which prompted deliberations about undergoing PSA screening myself. Below is a picture of my dad when he was 83 years old at his birthday party, 7 years after he was treated for prostate cancer with hormonal therapy and localized irradiation. He remains cancer-free in 2018.
I was 53 years old when I found out my dad had prostate cancer in 2006. I, like many men in our 50s and 60s, was faced with what to do about prostate cancer screening, and knew my dad had prostate cancer. The guidance from the U.S. Preventive Services Task Force was not clear during that time and I share the information as it evolved in the 2000s.
- In 2008, the U.S. Preventive Services Task Force concluded that the current evidence was insufficient to assess the balance of benefits and harms of prostate cancer screening, or an I Recommendation.
- In 2012, the year I ended up being diagnosed, the task force recommended against PSA-based screening for prostate cancer, or a D Recommendation.
- Now in 2018, the Task Force just recommended that for men age 55 to 69, the decision to undergo periodic PSA-based screening for prostate cancer should be an individual one. Before deciding whether to be screened, men should have an opportunity to discuss the potential benefits and harms of screening with their clinician, or a C Recommendation.
So, this advice has been bouncing around and did not give clear guidance to someone needing to make a decision, even someone firmly embedded in the field of cancer. Despite the uncertainty hovering around the prostate cancer screening, given that my dad had prostate cancer, my internist and I decided to have the PSA checked starting in my 50s.
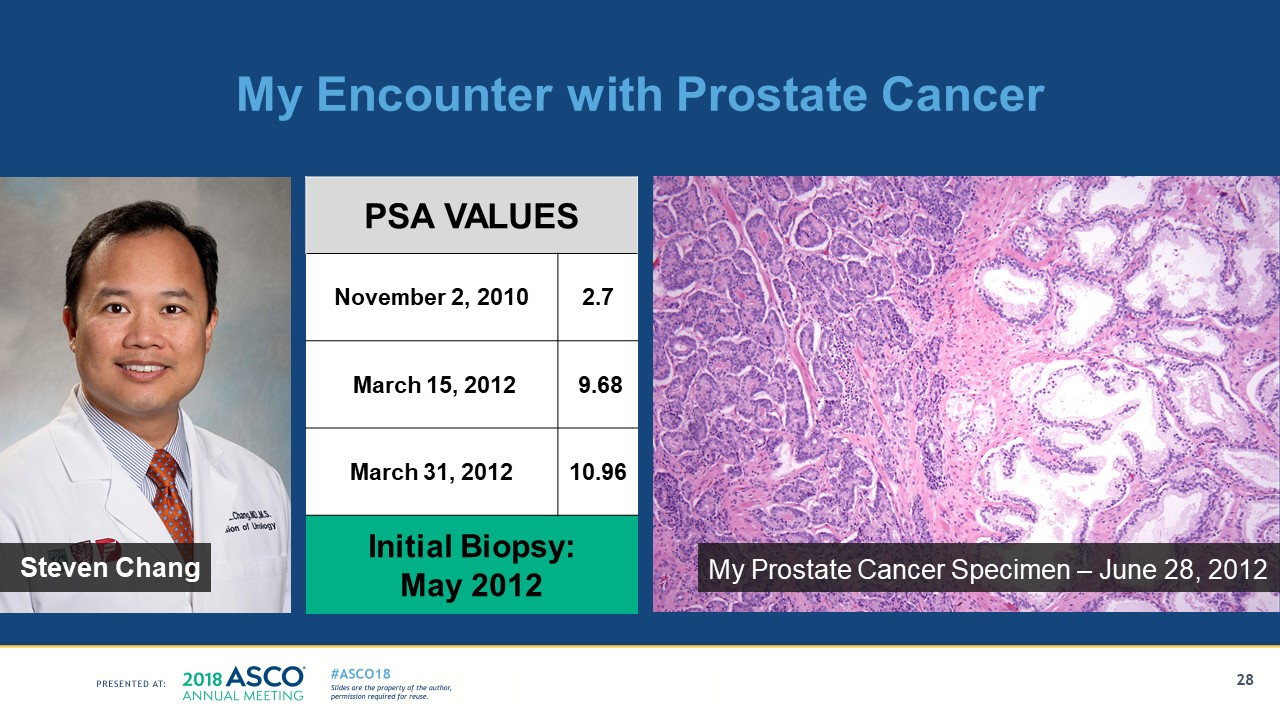
On November 2, 2010, when I was 57, my PSA was 2.7, below the upper limit of normal, 4.0. Then I went through what a lot of our patients go through. I signed on to my medical record on March 15, 2012, when I was 59, and saw it went from 2.7 in 2010 to 9.68 during my annual check-up.
I thought I needed to verify the elevation and checked it 2 weeks later, on March 31, and it continued to be elevated at 10.96. The biopsies were scheduled more than a month later, in May 2012, so I had to wait for more than a month not knowing my status and living with the uncertainty of a potential cancer diagnosis. One of six biopsies from the one side of the prostate showed prostate cancer involving of one of six cores. These findings pointed away from observation and toward therapeutic intervention, so I opted for a surgical resection. One has to wait for another 6 weeks after biopsies, so the operation was done on June 28, 2012, more than 3 months after the initial observation of a high PSA.
I have now personally experienced what it is like going for 3 months not knowing the eventual status of my cancer and trying to carry as normal a life as possible with the distractions of a cancer diagnosis hovering over my head, with the uncertainty about my future. During these 3 months, I was seeing patients in clinic, working on papers, and submitting grants. It was a challenge for me, as it is for many of my patients, to focus on my duties as an oncologist and academician. I was experiencing the uncertainty of what would be ultimately be found and the potential impact on my life and my expected survival.
My surgeon, Dr. Steven Chang, performed the prostatectomy and the resection yielded a stage II with my photomicrograph shown on the right of the slide below. As many of you know, a stage II cancer is neither the best nor the worst stage of cancer to have.
Similar to many of our patients, I have lived and continue to live with the uncertainty of whether my prostate cancer will come back. Now that nearly 6 years have passed, I feel blessed that thus far I have avoided many of the potentially devastating consequences of recurrent cancer.
The opportunity to give this address has made me think and document the things in my life that I could have missed had my cancer not been picked up and effectively treated. I have lived to see my son, Evan, get married in 2016, my daughter, Katherine, married in 2017, and our first grandchild born in 2017. You can see my grandson, Edward, and me in 2018, below. I also share the photograph of the gavel passing from Dr. Daniel Hayes to me at the 2017 ASCO Annual Meeting. I consider it one of the great honors of my life to be able to serve this year as ASCO President and to be delivering this presidential address.
I am grateful to have lived through this transformation of the treatment of many of our patients with lung cancer. As I think about this year’s theme, “Delivering Discoveries: Expanding the Reach of Precision Medicine,” we should all remain focused on what we hope to achieve for our patients.
I told you I was going to challenge you with a call to action, so that we can expand the reach of precision medicine. As clinicians and researchers at this pivotal time in cancer research and cancer care, we need to extensively characterize our patients’ tumors, treat them with our most effective agents, and support a robust research effort to improve the efficacy of the drugs. ASCO needs to continue to lead efforts to guide the selection of the testing needed for each type of cancer, provide point-of-care support for decision making, and generate information on the outcomes of the patients in the real world outside the academic centers.
I have seen and played a small role in the introduction of some of the four different FDA-approved targeted therapies and been able to successfully treat many of my patients with immunotherapy.
Given my own encounter with prostate cancer, I now have personal insights into the anxiety faced by many of our patients about the return of their cancer. I want to remind you, as we do our work and see our patients, we must be mindful of the roles we can play beyond selecting the appropriate therapy for our patients and see to the psychological needs of our patients as well. We must acknowledge the need to continue to innovate with our treatments from ongoing research to improve the lives of our patients. We must also be aware that our patients worry not only about the efficacy of our treatments but also that they do not want to miss the critically important events in our lives that we share with those around us.
I have been proud that I have lived to be able to serve as your President of ASCO.
Editor's note: Transcript has been edited slightly for style and clarity.
Comments
Raymond U. Osarogiagbon, FACP, MBBS
Jun, 09 2018 2:07 PM
Just watched this (having missed the live presentation), very profound, very moving. This needs to be disseminated to all oncologists all over the world and all physicians! Anywhere on earth. These perspectives are germane to everyone, everywhere...
Ray