Jun 01, 2016

ASCO President Julie M. Vose, MD, MBA, FASCO, and ASCO CEO Allen S. Lichter, MD, FASCO
Watch an exclusive video of Dr. Julie M. Vose delivering her Presidential Address at the 2016 ASCO Annual Meeting. Read the complete transcript of her address below the video.
By Julie M. Vose, MD, MBA, FASCO
2015-2016 ASCO President
It was truly an honor for me to announce the creation of the Allen S. Lichter Visionary Leader Award. What a fitting tribute to a legendary oncologist, breast cancer researcher, medical school dean and—over the past 10 years—insightful and innovative CEO for our organization. I know I speak for the staff and membership in saying how grateful we are for all you have done for ASCO.
And what better time and place to recognize those achievements than at ASCO’s 52nd Annual Meeting? I’m truly delighted to welcome our many members and friends who have come to Chicago from across the nation and around the world. We have a spectacular Annual Meeting underway. In 2016, we are welcoming 37,500 attendees from nearly every state in the union and more than 125 other nations around the globe. This year, we received more than 5,800 total abstracts and offered two different pre-Meeting programs of seminars and case-based courses. Plus, we are providing innumerable networking opportunities to share knowledge, gain insight, and improve cancer care.
The scale and scope of this meeting underscores the American Society of Clinical Oncology’s vital role as the world's leading professional organization for physicians and oncology professionals caring for people with cancer. I’m proud and truly honored to have had the opportunity to lead ASCO as its 52nd President during the past year. This has been a time of tremendous change and exciting developments in cancer care. It is both an enormous challenge and unparalleled opportunity to lead an organization like ASCO. It is a time that stands at the vanguard of scientific discovery and translating those advances into saving lives.
You can only be as effective as the people who support you, and in that regard I have been especially fortunate. I would like to thank Dr. Lynn Schuchter, Scientific Program Committee Chair, and Dr. Apar Ganti, Cancer Education Committee Chair, of the 2016 ASCO Annual Meeting, for their tireless efforts in putting together the exciting program this year and for their extensive support throughout my presidency.
In life, too, you can only be as effective as the people who support you. And in my own life I have been very fortunate. I dedicate my talk this morning to my parents, who so perfectly embody this Meeting’s theme of Collective Wisdom. My father is a pathologist. During summer breaks when I was a student, he gave me the wonderful opportunity to work in his lab. It was there, with his guidance and encouragement, that I first became interested in understanding cancer cells. My mother understood the necessity of following where your curiosity and passion leads and urged me to invest in myself with education. The collective wisdom of their guidance and thinking put me on a path of lifelong learning.

Pictured: Dr. Julie M. Vose (center) with her parents, Doris Vose and Dr. James Vose.
Collective wisdom supports and sustains me to this day. There is no greater source of it in my daily life than the lymphoma team at the University of Nebraska Medical Center. And this morning, I salute my friends and colleagues Dr. Philip Bierman, Dr. Matthew Lunning, Dr. Gregory Bociek, and Kathy Byar, APRN.
I especially want to recognize Dr. James Armitage. He has been my mentor and guide for more than 30 years. His insights and understanding on lymphoma care and research have improved the lives of countless patients. The wisdom he has gained in these encounters has made him an unparalleled mentor for many oncology trainees. The generosity with which he has shared his wisdom has made him an unmatched friend.
Around the world, every one of us working in the field of oncology strives each day to advance our knowledge and understanding of cancer. Through delivery of high-quality care, we lend comfort and aid to cancer patients and their families. ASCO is the world’s preeminent professional oncology society and is an invaluable aid and ally in all that we do. Not surprisingly, ASCO’s staff and leadership are some of the best in the world, with tremendous expertise in areas that touch every aspect of oncology. Over the years of my association with ASCO and now as President, I have come to hold them in respect and esteem. I wish to convey my gratitude and deepest appreciation for all they have done to make this past year successful, inspirational, and deeply rewarding.
Working with the ASCO staff and meeting members of this organization in locations around the world during the past year has highlighted the incredible depth of commitment to our mission. ASCO is a professional oncology society committed to conquering cancer through research, education, prevention, and delivery of high-quality patient care. These are the goals that all of us strive to achieve on a daily basis. We do it as we care for our patients, as we advance understanding through research and discovery, and by working to ease the burden of cancer on our society through policy and advocacy. ASCO’s members are at the front lines in the global fight against cancer.
ASCO is the very embodiment of collective wisdom. It is a diverse and multifaceted global organization representing over 41,000 members worldwide. Its membership is 33% international and its global presence continues to expand. This year, ASCO is proud to welcome a record number of attendees from across the globe.
At the same time we celebrate these international connections, we also recognize how vitally important they are becoming in the context of global health. According to the World Health Organization, cancer is already among the leading causes of morbidity and mortality worldwide, and the number of new cases is expected to rise by about 70% over the next 2 decades (Figure 1). Today, about a third of cancer deaths are due to the five leading behavioral and dietary risks, with tobacco use the most significant risk factor. This growing global cancer burden will be a defining human health story in the 21st century.

Figure 1. Predicted worldwide cancer cases and cancer deaths.
To address cancer care globally, ASCO has many international educational meetings and programs. In just this past year alone, we have organized 23 courses and symposia in countries ranging from Brazil to Zimbabwe, as well as the Best of ASCO® International meetings in 25 countries. ASCO also has ongoing capacity-building programs in Honduras, Vietnam, Bhutan, and soon Nepal and Ghana. We support sponsored research in Nigeria, Uganda, Mexico, India, and Romania. We have also recently launched the Journal of Global Oncology, and the Quality Oncology Practice Initiative, or QOPI®, is also available as an international program.
As ASCO expands these programs, we will continue to find new ways to support oncology health care providers globally in advancing cancer prevention, education, and quality care.
Here at home, while cancer incidence in the U.S. has declined over the last decades, the overall number of cancer cases has not. Due to the aging of the U.S. population, the total number of patients with cancer continues to rise. Over the next few decades, we can expect what has been described as a “tsunami” of cancer patients due to this effect.
The question must be asked: Are we ready to care for these patients?
Here again, the importance of a strong national and international organization working and advocating on behalf of oncologists and their patients cannot be overstated. Two years ago, when ASCO surveyed the oncology workforce, it estimated that within the next 10 years, demand for medical oncology and radiation oncology services will grow by 40%, while the physician workforce to provide these services will only grow by 25% (Figure 2). That leaves a projected shortfall of approximately 2,400 hematologist/oncologists and radiation oncologists just in the United States alone.

Figure 2. Oncology workforce projections.
The International Agency for Research on Cancer estimates that by the year 2030, nearly 22 million new cancer diagnoses and 13 million cancer deaths will occur around the world each year. When we hear such numbers, or talk about a cancer “tsunami,” it is easy to feel overwhelmed. But as we all know, cancer is an intensely personal disease. It occurs one person and one life at a time. We have dedicated our professional careers to enhancing the lives of patients and families dealing with a cancer diagnosis. Knowing that our work can make such a difference in their lives is profoundly rewarding in our own lives.
A true delight of my year leading ASCO has been the opportunity to travel and meet oncologists and researchers who work in so many different locations around the world. My fellow Omaha, Nebraska, native Warren Buffet has many famous sayings about business and investing. I find they often apply far beyond finances. For instance, he once said, “Someone's sitting in the shade today because someone planted a tree a long time ago.”
For ASCO, that tree was planted back in 1964, with a meeting here in Chicago of seven top oncology leaders. Just as today, they came together with a common concern for patients with cancer. They had the powerful insight that working together across distances and across disciplines, we could achieve our mission to have a world free from the fear of cancer. The conviction that by working together, we could cure cancer, began to take hold. What started as the vision of seven individuals soon became a call to the nation. All of us here today sit in the shade of a remarkable half century-plus of previous ASCO members who have advanced cancer care and treatment to a level today not imagined in 1964.
It is difficult today to fully appreciate the foresight and bravery of ASCO’s founders. We find it hard to remember or even imagine a time when cancer was such a dreaded disease that people simply refused to talk about it, a time when it wasn’t cancer, but “the big C.” In answer to a questionnaire administered in 1961—just 3 years before the first ASCO meeting—fully 90% of responding physicians indicated a preference for not telling a cancer patient his diagnosis. Imagine 90% of us here today being reluctant to tell our patients the disease they were facing!
It was the tremendous dedication of those early ASCO pioneers—whose soaring aspirations we all share today—that gave birth to a movement that transformed cancer from the disease you did not talk about, to the disease that demanded a cure.
In 1971, it led President Richard Nixon, appearing before Congress in the State of the Union address, to declare a “national commitment” to cure cancer. Cancer came out from the shadows. The results were profound. Just 6 years later, a new survey found 97% of physicians indicated they’d prefer to tell a cancer patient his diagnosis—a complete reversal of attitude.
But in the 45 years since President Nixon set the national goal of beating cancer, we have learned that cancer is not one disease, but many. It is not one problem, but a whole host of incredibly complex processes that work in tandem. For scattered individuals working alone, it’s an impossible task. Solving cancer requires not one approach or one discipline of knowledge, but the collective wisdom of many.
In the 21st century, fighting cancer has truly become a team effort. The evolution of the Internet has connected researchers across great distances and national boundaries. It has also facilitated the rise of patient advocacy communities, transforming cancer patients from passive subjects of their treatments to active participants and decision makers. This has made a world of difference in all aspects of cancer research and care, from diagnoses through treatment and on to survivorship.
The advent of multimodality patient care teams, comprised of physicians and health care professionals who specialize in specific types of cancer, has shown how we can reduce time between diagnosis and treatment. This has streamlined the maze of referrals, tests, treatments, and specialists, while increasing the likelihood of long-term survival for our patients.
This new understanding of how we will succeed in beating back cancer has led to a new confidence, and a new excitement, that I have seen again and again as I have traveled the country and the world on behalf of ASCO.
Most notably, this new burst of discovery and possibility was recognized in January when President Barack Obama turned to Vice President Joe Biden at the State of the Union address and asked him to lead a cancer "Moonshot" task force—and the Vice President made it clear he was ready to take on the job. We are very fortunate that Vice President Biden will be addressing us during a Special Session on Monday about his vision.
The theme of my year as ASCO’s President has been “Collective Wisdom: Patient-Centered Care and Research.” In particular, I wanted to highlight the importance of multimodality care, and how it benefits our patients. Day-to-day work within cancer specialties and through new areas of scientific inquiry is constantly enhancing our collective wisdom, which in turn shapes the future of patient care. As our understanding grows, we continually need to incorporate new areas of expertise to transform how cancer care is delivered. Quality care will increasingly be understood to include advanced practice providers and other patient care specialists to meet patients’ evolving care needs.
The second part of my theme—Patient-Centered Care and Research—signifies the importance of this need. By concentrating our efforts around the patient’s needs for cancer treatment, supportive care, as well as survivorship care, we will be able to learn from every patient today in order to help the cancer patients of tomorrow. That is the value of collective wisdom.
I have another favorite quote from the Sage of Omaha, Warren Buffett: “Price is what you pay, but value is what you get.” If we face a cancer tsunami, if globally there will soon be more than 20 million new cancer diagnoses each year, then our focus must be not on simply more treatments, but on delivering more high-value quality care. This is why so many of the sessions at this Meeting are designed to provide information on the value of cancer care in conjunction with the scientific and medical information. ASCO programs focus on every aspect of improving cancer care and supporting the oncology health care team.
In this context, I believe it is better to show rather than tell. In order to demonstrate how ASCO programs assist us every day in our practices and how they can directly support our patients, I would like to present a hypothetical patient case that illustrates many of the ways that ASCO programs support us.

“Mary” is a 65-year-old patient who presents with abdominal pain and diffuse lymphadenopathy. A biopsy of a supraclavicular lymph node demonstrates diffuse large B-cell lymphoma. She has stage IIIA disease. This is our patient. She presents to you for an opinion on the best therapy and what her prognosis would be.
Mary is offered participation in a federally funded clinical trial, which is a large intergroup trial with the results still pending. This trial randomized patients to receive R-CHOP or dose-adjusted EPOCH-R and had associated genomic testing to further classify the lymphoma by molecular profiling (Figure 3). Although the trial has completed enrollment, results are not yet available.

Figure 3. CALGB 50503 schema.
Mary’s case clearly captures the need for clinical trials. For her diagnosis, there are varying treatment options, but the best treatment is not known. This type of study—a large intergroup trial that compares two standard-of-care regimens—could not be conducted outside of a federally funded research study. The model of coordinated national research that was first launched by President Nixon more than 4 decades ago remains today the most powerful engine for making advances in our understanding and treatment of cancer. This is why ASCO is a leading national advocate for increased funding for the National Cancer Institute [NCI]. The federal government has a vital role to play in bringing important cancer research and clinical trials to our patients. We were especially pleased and grateful this year for the increased National Institutes of Health budget of $2 billion. More money for more trials is vitally important. At the same time, we will continue to advocate for enhancements in the current cancer clinical trials system.
We believe there is room for streamlining the clinical trials process to increase the number of patients on clinical trials, decrease the cost of trials, and accelerate the time to completion. We need our clinical trials process to be a lean, mean, cancer-fighting machine. Over the past year, ASCO took a leadership role in identifying and promoting useful changes. Along with the Association of American Cancer Institutes, we hosted a workshop on “Best Practices in Clinical Research,” bringing together 62 individuals, including cancer researchers, research nurses, regulatory specialists, and contracting specialists. Additional attendees included representatives from the pharmaceutical industry, contract research organizations, the Food and Drug Administration, the National Cancer Institute, and patient advocates.
Prior to the meeting, we surveyed a large number of stakeholders, looking to identify areas that could be optimized to enhance clinical trial goals. This effort continues. We are focused on finding and implementing significant new efficiencies in clinical trial methodology. This will be a multiyear project for ASCO, working across the clinical trial research community, in addressing the highest priority issues for optimization.
But this is the current reality we face. Here in the United States alone, despite more than 1.6 million cancer diagnoses expected in the coming year, just 3% of adult cancer patients will enroll in clinical trials. Often, they are not representative of the types of cancer patients we see every day in our clinics, patients who tend to be older with significantly more comorbidities. Think of it: 97% of adults don’t go on clinical trials. These are the missing pieces of the puzzle.
How can we learn from these real-world patients?
In our model patient Mary’s case, information on clinical outcomes of patients treated within the trial are not yet available. Others have faced similar experiences. The problem is that there has been no coordinated and systematic effort to record, trace, and share that information.
Until now.
CancerLinQTM is live and it is real. Although results of the NCI-sponsored trial that our patient Mary participated in have not been reported to date, thanks to CancerLinQ we can tap into the wisdom of our colleagues across the country. In order to learn from prior patients with similar characteristics, we enter similar patient characteristics into the CancerLinQ rapid learning system and evaluate current patterns of care of two types of chemotherapy in the trial.
As Mary starts her treatments, like many patients, she seeks out additional education on her lymphoma subtype, the treatment she will be receiving, as well as the potential side effects. At the advice of her cancer team, Mary turns to Cancer.Net, ASCO’s award-winning patient information resource. The site has a vast amount of patient- and family-directed educational materials covering all aspects of patient and caregiver education.
After treatment begins, Mary experiences the expected toxicities associated with her therapy. However, her physician had just attended the ASCO-cosponsored Palliative Care in Oncology Symposium, where she learned the most up-to-date information about treatment of chemotherapy-induced nausea, vomiting, and neuropathy. Based on this information, modifications of Mary’s supportive care regimen lead to a marked decrease in these toxicities. The Palliative Care in Oncology Symposium is an excellent example of ASCO’s focus on patient-centered care and research. We first began offering the Symposium in 2014 to enhance oncology health care providers’ knowledge of supportive care measures in order to better assist patients before, during, and after therapy.
Mary’s oncologist already had direct experience with the professional benefits available through ASCO. Previously, she was the recipient of ASCO’s Young Investigator Award, which enabled her to gather preliminary data, which in turn led to her being awarded an NCI grant on clinical and translational research. This program has supported 945 Young Investigator Awards over the past 32 years. Today, 98% of the awardees remain active in the field of oncology research. For Mary’s oncologist, like many others, the award came at an important juncture in her career.
The Conquer Cancer Foundation of ASCO makes grants and awards to support clinical and translational cancer research done by gifted physician-scientists at every stage of their careers. From the best and brightest among young investigators to senior researchers providing mentorship opportunities for the next generation of cancer researchers, this support has provided crucial impetus to advance understanding and improve care. To date, we have presented more than $100 million in grants and awards to over 1,500 promising oncology researchers.
Mary was also very fortunate to be treated in an oncology practice that is QOPI Certified. The Quality Oncology Practice Initiative Certification Program provides a 3-year certification for qualifying hematology-oncology practices promoting safety and advancing best practices. Quality measures developed by world-renowned practicing oncologists and quality experts, employing clinical guidelines and published standards, are continually re-assessed to maintain rigor. QOPI provides a systematic process, a library of diverse quality measures, data collection tools, and reliable information to assess the care provided.
The treatments in Mary’s trial may not only have different outcomes, but also different toxicities and costs. ASCO’s Value Framework, first published last year, takes into account outcomes of the treatment such as response rate, progression-free survival, and overall survival, as well as toxicities of the therapy. Studies have shown that when faced with questions regarding financial information, medical effectiveness, and treatment toxicity, patients want to talk to their doctor. The Value Framework brings together information on effectiveness, toxicity, and cost so that patients like Mary can discuss with their physician the net health benefit of a given drug regimen when compared to a standard of care.
Since the trial our patient Mary was on is not yet reported, these results are hypothetical, demonstrating the possible differences in toxicity, clinical benefit, and cost. In this example, regimen A demonstrated a slight improvement in progression-free survival with a similar toxicity compared to regimen B. This results in a small improvement in the Net Health Benefit for regimen A. However, an additional factor: The cost of regimen A is significantly higher than regimen B (Figure 4).

Figure 4. Hypothetical clinical benefit, toxicity, net health benefit, and cost comparison between therapy regimens.
This type of analysis is designed to be used at the point of care to assist the physician’s discussions with the patient and family. The Value Framework has been recently updated to take into account the many comments received during the open comment period. ASCO’s goal is to have an effective user-friendly program that can help in discussions with patients at the point of care for informed decision making.
As oncologists, we are experienced in delivering treatments in a health care environment that is constantly changing and advancing. But one area where consistency and reliability are critical is in reimbursements. ASCO, along with countless other stakeholders, has worked for years to try to repeal Medicare’s Sustainable Growth Rate, or SGR, for physician reimbursement. We were pleased and optimistic when SGR was finally repealed last year. However, we must now educate ourselves on the new initiative: the Medicare Access and CHIP Reauthorization Act, or MACRA.
MACRA is intended to move more quickly toward Medicare’s stated goal of paying for high-value care. It enables health care providers to take part in one of two quality programs: the Merit-Based Incentive Payment System, or MIPS, or participation in an Alternative Payment Model, or APM. Both MIPS and APMs will go into effect in 2019, but 2017 will be the baseline for measuring and scoring physician performance.
The MIPS program will streamline existing performance reporting programs—the Physician Quality Reporting System (or PQRS), Meaningful Use, and the Value-Based Modifier—into a new performance measurement program with one score for all components.
Looking ahead and recognizing that we would be migrating from fee-for-service medicine to quality- and outcomes-based medicine, ASCO assembled a large task force which developed the Patient-Centered Oncology Payment Model, or PCOP. The ASCO PCOP model decreases avoidable costs such as hospitalizations, emergency room visits, and excessive treatments and tests, while shifting and enhancing the support of needed services such as case management and coordination. Our treatments are only as good as our ability to deliver them to patients, so it is imperative that we respond nimbly and effectively to today’s changing health care system.
Even in the best of circumstances, though, some medical procedures prove ineffective. In Mary’s case, unfortunately, she has a relapse of her lymphoma a year later. But new options for treatment based upon genomic or protein biomarkers are broadening treatment options. As we learn more about the drivers of cancer, genomic profiling has become more informative. Precision medicine is becoming a reality.
Mary has a genomic analysis performed on her lymph node biopsy, which demonstrates an atypical ALK fusion. Although some patients are being treated off clinical trials based upon this genomic information, the needed medications may not be available and information from the treatment would not be available to help future similar patients.
Our patient Mary was enrolled on ASCO’s first clinical trial, the Targeted Agent and Profiling Utilization Registry Study, or TAPUR. In this trial, a participating clinician can match a patient’s genomic test to an FDA-approved targeted drug through an automatic matching process. If the match is not straightforward or the clinician requests guidance, a Molecular Tumor Board is available to evaluate the patient’s case. There are currently 16 drugs for 15 therapies, with two of the therapies involving drug combinations, which pharmaceutical companies have provided for the study. ASCO opened a few pilot sites in March 2016 and will expand to a second wave of study centers over the next few months.
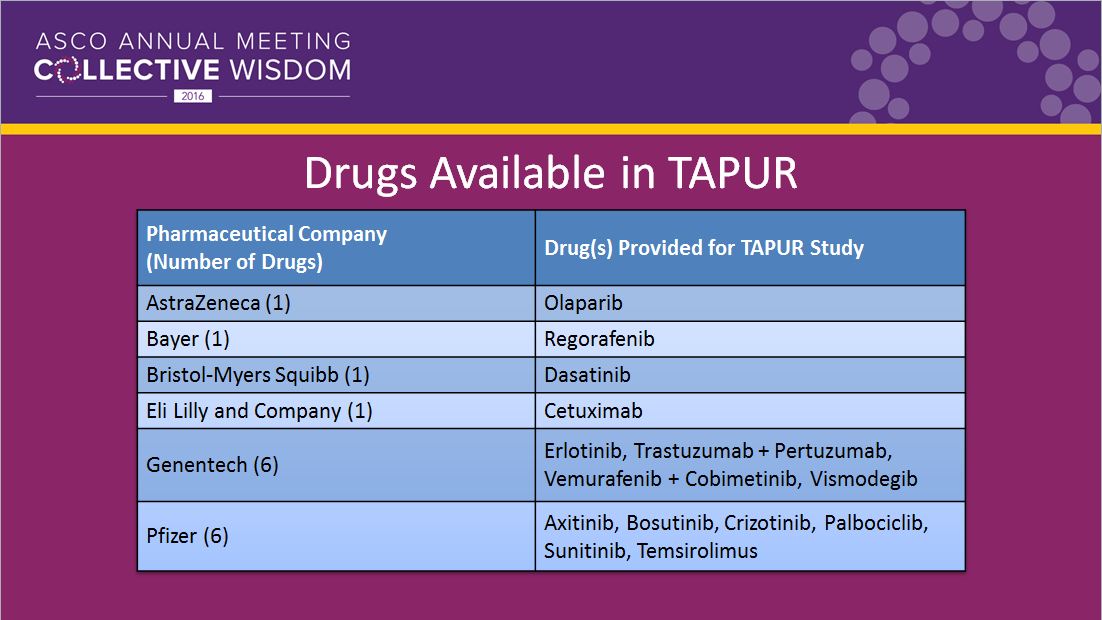
Figure 5. TAPUR study drugs.
These are the drugs currently being provided by the listed pharmaceutical companies on the TAPUR trial (Figure 5). Additional agents will be added over time as they are made available. Patients will be evaluated by standard response criteria. Higher grades of toxicities and clinical outcomes will be collected on the trial evaluation by tumor type as well as molecular genomic abnormality. This study will allow the collection of real-world data for patients treated with matched agents in this precision medicine targeted clinical trial.
Mary’s outcome is a happy one. She has a complete response to the therapy provided in the TAPUR study and becomes a long-term survivor from her relapsed diffuse large B-cell lymphoma.
Every day, there are more and more patients like Mary. Cancer survivorship is more than just a term; it is a growing movement, and many more will be survivors as future therapies evolve. The Institute of Medicine estimates that in the United States alone, there will be 20 million cancer survivors by 2025. We will need to assist these survivors and their families on their journey with new research, new education, and new understanding of survivorship issues.
Here again, ASCO is taking a leading role by addressing this with a new Cancer Survivorship Symposium, with a goal of improving the health care of cancer survivors. This meeting is co-sponsored with the American College of Physicians and the American Academy of Family Physicians. The initial meeting, held last year, was something of a first, with its patient-centered focus after cancer. The creation of the Symposium underscored ASCO’s commitment to cancer survivorship. It is the next step in expanding survivorship information for oncologists, including expanded clinical guidelines, a survivorship care plan template, and survivor resources on Cancer.Net.
Continuing education for practitioners remains an important priority for ASCO. In addition to this Annual Meeting, we now have six thematic meetings each year, including the Cancer Survivorship Symposium, Quality Care Symposium, ASCO Oncology Practice Conference: The Business of Cancer Care, and the new ASCO-SITC Clinical Immuno-Oncology Symposium. All of these educational meetings—as well as the ASCO University® online education and Cancer.Net—assist both oncology health care practitioners and patients and their families in obtaining the most up-to-date knowledge available on oncology-related topics.
The original founders of ASCO would doubtless be proud—and amazed—at what has been accomplished over the last 52 years. No doubt they would be astonished at the scope and size of today’s ASCO, with over 41,000 members and an international organization comprised of 16 departments. Every year, ASCO staff and hundreds of volunteers continue to make improvements for the future of cancer care, research, and education. At ASCO’s first scientific meeting held in Chicago in 1964, 51 attendees planned the following year’s meeting. Now in 2016, we are already looking forward to hosting nearly 38,000 attendees here in Chicago at this year’s Annual Meeting. What an accomplishment for our Society!
As we go forward into the 53rd year of ASCO, I would like to welcome Dr. Dan Hayes as the next President of ASCO and Dr. Bruce Johnson as President-Elect. These are two exceptional leaders in the field of oncology, and I know ASCO will be well served by what they bring to moving us forward together.
I would like to again thank Dr. Allen Lichter for his visionary leadership over the past decade. His guidance has allowed ASCO to stay on the cutting edge of professional societies. On a personal note, Allen has also been a wonderful friend and mentor for me as well as many previous ASCO Presidents.
I know I speak on behalf of the staff and the entire membership of ASCO in welcoming and applauding Dr. Clifford Hudis, who will be ASCO’s new CEO starting at the end of June 2016. With Dr. Hudis at the helm, ASCO’s future will continue to be very bright for decades to come.
I hope that over the next 50 years of ASCO, future oncology health care providers and researchers will look back and be proud of what we have accomplished for cancer research and patient care. It has been my great honor to serve at the head of an organization that has an illustrious history, a vital role in cancer advocacy, research, and care, and a truly bright future in helping lead us to the day when we can meet and defeat cancers of every type.
Editor's note: Transcript has been edited slightly for style and clarity.
Comments
Jayaprakash Madhavan, MD
Jun, 12 2016 8:10 PM
I am following ASCO 16 here In India. It an excellent scientific meeting. the presedential address is very encouraging. patient centered oncology practice very important every where especially in countries like India where resources are less. Hope that India is also involve in Moonshot initiative and collective wisdom. ASCO should encourages more exchange programmes so that ecellent patient centred care and clinical research to conquer cancer
Dr jayaprakash Madhavan, Sr consultant Oncologist and head Kims Pinnacle Comprehensive cancer Center Trivandrum kerala India