

Dr. Sabesan.
By Sabe Sabesan, PhD, FRACP
Growing up in a village in Northern Sri Lanka, befriending rural Australians in medical school at Flinders University in Adelaide, and doing my internship in Alice Springs provided me lived and observed experience of the enduring daily difficulties in accessing health services faced by regional and rural communities. Negative experiences of regional and rural communities and their health workforce and the accumulating evidence indicating poorer health outcomes among these communities is a call to action for policymakers, health managers, and health care professionals.
In 2004, my family moved to a large regional town, Townsville, in North Queensland, which is the tertiary hub for a population of nearly 1 million over a land mass of almost 2 million square km; pretty dispersed, right? Our dedicated team of medical oncologists and administrators began rolling out a tele-oncology model as the foundation for enhancing care closer to home. We quickly realised the priority was to shift specialist services to rural towns using a tele-oncology model that allows chemotherapy administration (tele-chemotherapy),1 shared care with rural practitioners and tele-supervision arrangements, and consequently building rural capabilities and broadening scope of practice. This contrasts with fly-in-fly-out outreach services and tele-oncology consultative services that usually do not leave expertise in or transfer expertise to rural towns. Many of the current decentralized clinical trial models are focusing on oral medications only, bypassing rural hospitals and dealing directly with patients, ignoring the fact that it will be difficult to build and sustain rural capabilities and scope of practice without involving rural health facilities.
If we can provide chemotherapy services through a tele-chemotherapy model at smaller rural centers, why can’t we do the same for clinical trials? After all, clinical trials improve cancer outcomes, and they should be offered as an option for all patients with cancer. Most rural and regional centers don’t have trial units or a trial culture/infrastructure, citing a variety of barriers to implementation. Ultimately, it is an unethical and non-compassionate health practice to disadvantage a group of vulnerable citizens based on geography. We cannot just leave equity within the remits of a handful of bureaucrats, clinicians, health managers, and management consultants. This is where a national and state-wide system approach to health equity becomes imperative.
National reforms in clinical trials require national advocacy levers. The main advocacy lever we have in Australia is the Clinical Oncology Society of Australia (COSA), which offers clinicians a credible national platform to co-design models of care, develop national frameworks, and ultimately effect policy changes at government levels.
We chose the Australasian Teletrial Model (ATM) as the tool for connecting regional and rural sites with metropolitan sites to form trial clusters so that some or all aspects of clinical trials could be offered closer to home (Fig. 1). The primary site and satellite sites become collaborative trial clusters, guided by mutually agreed supervision plans that articulate how duties are delegated within the cluster.
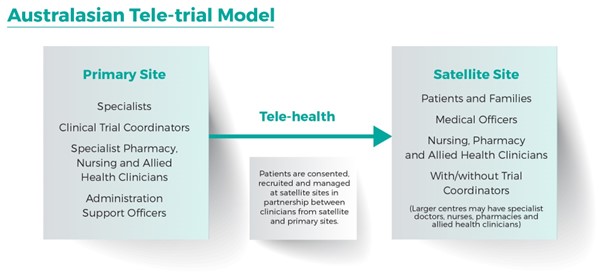
Figure 1: Schematic representation of the Australasian Teletrial Model (COSA Australasian Teletrial model: National guide for implementation 2016)
Partnering with Medicines Australia, Australian Clinical Trials Alliance, state governments, and cancer centers, COSA produced the ATM: National Guide for Implementation in 2016. A subsequent pilot project through the COSA Teletrial Consortium informed the development of national teletrial principles and standard operating procedures by the Commonwealth Health Department2 and all states and territories. This also delivered a business case for an AU$100 million national program led by states and territories. This program aims to build regional clinical trial coordinating centers in each state and territory, to remove bureaucratic burden on the clinical workforce, and to offer recruitment boosting funds, seed funds for trial coordinators, and education and training. One major component of the program is to initiate and effect reforms in ethical and regulatory approvals, to be patient- and workforce-centered.
The program is meeting its timelines by creating trial clusters in many fields of health care (not just oncology), partnering with many sponsors to adopt the teletrial model, harmonizing national and state policies, upskilling many clinicians on this new paradigm, and achieving some early wins in regulatory reforms. However, it has become evident that faster implementation and sustainability of the program requires whole of system ownership and a reform methodology (the System Lasagne model)3 rather than only relying on the bottom few layers of the system in the usual pyramid model of health system arrangement. In a System Lasagne model, all layers of the health system (government department to the frontline workforce) are aligned with the strategic purposes of the system and adopt actions to enable the layers below to deliver cost effective and high- quality services to consumers.
In a pyramid model, simply because of the shape of the pyramid, when governments pour taxpayer funds into it, significant wastage is a guaranteed and well-reported phenomenon. If we then follow the reform or System Lasagne methodology, the following actions may ensure the model of care is embedded at all layers and components of the system:
- All layers of the lasagne (or lasagna)—from government departments, health services, and clinical sites—need to drive the teletrial model as the solution for “equity of access” through new policies and procedures, regulatory reforms, performance measures, resource allocation, and reinvestment to grow the trial sector.
- Global and national sponsors need to mandate the teletrial model as a recruitment methodology, expect principal investigators to adopt trial clusters, and reform their internal processes, if they aspire to provide equitable access to all citizens.
- Ethics committees should mandate these kinds of models since equity and social justice are ethical attributes to expect from health systems.
It is pleasing to observe that Canada and New Zealand have adopted a teletrial model as their national model for decentralizing clinical trials into regional and rural communities so that all citizens can gain access to clinical trials closer to home regardless of post code or zip code.
Professor Sabesan, a senior medical oncologist at Townsville Cancer Center in Queensland, Australia, and a regional and rural system innovator, is the president-elect of the Clinical Oncology Society of Australia (COSA) and the clinical director of the Australian Teletrial Program-Queensland Department of Health. He serves on the ASCO Breakthrough Regional Committee. Follow him on Twitter @Sabesan68. Disclosure.
References
- Queensland Remote Chemotherapy Supervision Guide (QReCS). State Department of Health. Brisbane, Queensland, Australia. 2019.
- Australian Government Department of Health and Aged Care. The National Teletrials Compendium. 26 Feb 2021; updated 14 Feb 2023. Available at: https://www.health.gov.au/resources/collections/the-national-teletrials-compendium.
- Sabesan S, Kirk M. Health systems run differently: Flatten the pyramid and try something new. The Health Advocate. Nov 2022:22-24. Available at: https://issuu.com/aushealthcare/docs/the_health_advocate_november_2022.
Recent posts